

Abstract
Background: Hematopoietic stem cell transplantation (HCT) is a primary treatment option for various inherited metabolic diseases (IMDs). Successful engraftment is crucial for favorable survival and functional outcomes and correlates with optimal conditioning in these patients with an intact immune system. Traditional regimens have used myeloablative Busulfan and Cyclophosphamide (BuCy) which is associated with significant potential morbidity. Alternate reduced toxicity regimens, like Busulfan and Fludarabine (BuFlu), are often utilized to reduce treatment related toxicities.
Objective: To compare outcomes and complications with BuCy and BuFlu based conditioning regimens in patients with IMDs.
Methods: This is the largest single institution retrospective analysis of University of Minnesota's transplant database for patients with IMDs who underwent HCT using BuCy + campath or BuFlu + ATG based preparative regimen from March 2008 to September 2017. Incidence of neutrophil and platelet recovery were determined using standard definitions. Complications such as graft failure, sinusoidal obstruction syndrome, hemorrhagic cystitis and respiratory failure were compared. Graft failure includes primary aplastic graft failure, primary graft failure with autologous recovery, secondary aplastic failure and secondary graft failure with autologous recovery. Incidence of viral infections post-transplant comparing two regimens were also determined.
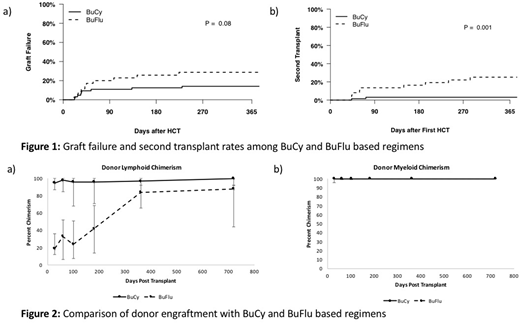
Results: Total of 99 patients were studied who underwent HCT for IMDs during the study period. Sixty-four received BuCy conditioning and 35 received BuFlu. Hurler syndrome (46%) and adrenoleukodystrophy (43%) were most common IMDs transplanted and umbilical cord blood was the most common donor source (74%). One-year overall survival was similar in both groups (81.2% in BuCy vs. 85.5% in BuFlu; p=0.8) with a similar incidence of grade 3-4 acute GVHD (9% in BuCy vs. 6% in BuFlu; p=0.5) and chronic GVHD (9% in BuCy vs. 7% in BuFlu; p=0.67) in the two groups. Neutrophil and platelet recovery were similar in both groups with significantly shorter duration of hospital stay noted in BuFlu group (median 21 d vs. 34 d, p = 0.002). The cumulative incidence of graft failure was higher with BuFlu conditioning (29% vs 14%, p= 0.08, Figure 1a). Significantly higher rates of second HCT was noted following BuFlu conditioning (27% vs. 3%, p= 0.001; Figure 1b). The incidence of adenoviral infection (14% vs. 0%, p=0.02) and hemorrhagic cystitis (23% vs. 3%, p=0.01) were notably higher in the BuCy group. Though donor myeloid engraftment was similar in both groups, donor T-cell engraftment occurred sooner with BuCy conditioning until 1-year post transplant (Figure 2).
Conclusions: Reduced toxicity conditioning leads to lower rates of infections and other transplant related complications, but is associated with a high rate of graft failure in patients with IMD. Alternate immune suppressive agents should be considered to reduce graft failure and minimize toxicities. Alternate donor options, including expanded UCB, should also be considered to improve engraftment in patients with IMDs.
Shanley:Magenta Therapeutics: Research Funding. Miller:Sangamo Therapeutics: Employment. Orchard:Magenta Therapeutics: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal